Study to examine Gastric Bypass for treatment of diabetes in non-obese patients
Gastric bypass surgery to treat diabetes in non-obese patients?
New York, NY
New York, NY
Patients with a body mass index below 35 generally do not qualify for weight loss surgery. But, researchers at Weill Cornell Medical Center in New York City are embarking on a new study to determine whether gastric bypass surgery can be an effective treatment for type 2 diabetes in people who are overweight but not obese.Gastric Bypass Malpractice Lawyer
The study aims to explore the correlation of diabetes and clinical obesity. Lead researcher Dr. Francesco Rubino notes that many people with a lower BMI can develop diabetes, and likewise, that someone who is severely obese could be diabetes free.
“For this reason alone, we need to start questioning whether BMI should be the only clinically appropriate way to decide who gets diabetes-targeted surgery,” Dr. Rubino said in a recent press statement. Diabetes affects more than 200 million people worldwide, and several studies have demonstrated that gastric bypass surgery can lead to spontaneous improvement or even resolution of the disease.
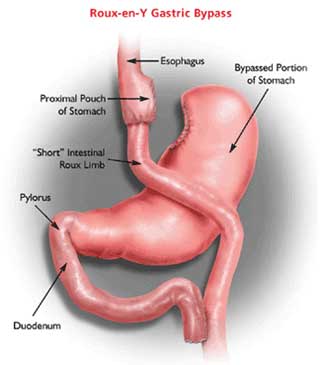
Dr. Rubino generally performs the standard Roux-en-Y bypass procedure in patients with a BMI over 35. Now, the potential benefits of the procedure are being extended to 50 non-obese patients as part of the current study.
Labels: gastric bypass diabetes, gastric bypass research, weight loss surgery business