Heavier patients carry increased risk in gastric bypass and other bariatric surgery
Higher risk for heavier patients in bariatric, gastric bypass surgery
Chattanooga, TN
Chattanooga, TN
For someone who weighs more than 500 pounds, the options for reaching a healthy weight can seem slim, but local bariatric surgeons say there is hope.Gastric Bypass Surgery Malpractice Injury and Wrongful Death Lawsuits
Dr. Jaime Ponce, medical director of bariatric surgery at Chattanooga's Gastric Band Institute, said special measures must be taken to operate on patients classified as super-obese and super-super-obese -- who have a body mass index above 50 and 60, respectively -- but it can be done.
"You have to take a totally different approach," Dr. Ponce said.
That means measuring to ensure the patient can fit on the operating table, working in a hospital certified to handle such patients and putting the person on a strict diet before surgery, he said.
Dr. Ponce performs about 300 bariatric surgeries each year, and he said 25 percent of those are on patients who have a BMI above 50.
Before the procedure, it's essential the patient is clear on what to expect from the experience, he said. Weight loss results often are less in patients with BMIs above 50, compared to those who are in the 35 to 45 range, Dr. Ponce said.
"They need to understand there is more risk," he said. "Every time the BMI goes up, there is more risk of bleeding because you're pulling fat to be able to see, and fat can start bleeding. There's more risk of damaging internal structures, more risk of having a breathing problem when trying to put the patient to sleep."
Despite the increased danger, for some patients the rewards are worth the risks.
Ducktown, Tenn., resident Sonya Standridge, 38, became one of Dr. Ponce's patients two years ago when she had Lap-Band bariatric surgery. She had a BMI of 63 before the surgery, which has dropped to 34 since the procedure.
With the Lap-Band, a small silicone tube is fastened around the upper stomach to create a tiny stomach pouch, slowing digestion and making the person feel full with less food.
Ms. Standridge said she has good days and bad days, but ultimately the surgery was the right choice for her. Being a nurse, she said she knew the risks beforehand and felt it was her "last resort option."
WHAT IS BMI?
Body mass index is a measure of body fat based on height and weight that applies to both adult men and women, according to the U.S. National Institutes of Health.
"If you asked me today would I have the surgery again, the answer is absolutely, 100 percent, no questions asked," Ms. Standridge said. "I had never felt the feeling of fullness before, so I would literally eat until I was gluttoned."
Local bariatric surgeon Dr. Jack Rutledge said there are two main factors that put high BMI patients at a greater risk than other patients.
The first, he said, is that people who fall into that category generally are unhealthy. Secondly, the additional weight creates a situation where it is more difficult to move instruments inside the body.
What he suggests to patients who are super-obese or super-super-obese is to first lose weight.
"I think they do have hope, but it's going to be expensive and it's going to be complicated," Dr. Rutledge said. "But there is a way to lose 100 pounds."
That's what 50-year-old Rossville resident Jimmy Allmond is trying to do now. After being told the increased risks of performing procedures on his 510-pound body, he decided to try to lose weight the old-fashioned way.
But he's still not sure on whether he'll eventually have surgery.
"With all that going on, I'm still not sure," he said. "If I can lose it without it, that would be good."BARIATRIC SURGERIES
* Gastric band: A ring is fastened on the top of the stomach, creating a small pouch. The ring has a balloon portion that can be filled with fluid to limit the amount of food the patient can eat. The apparatus acts as an hourglass, and food sits on top and slowly trickles down into the stomach. This is the least invasive of the bariatric surgeries.
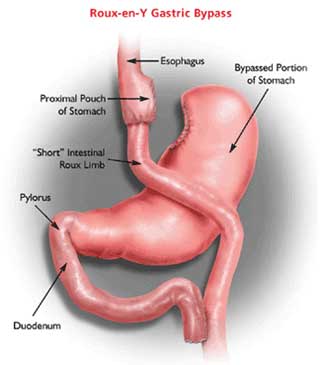
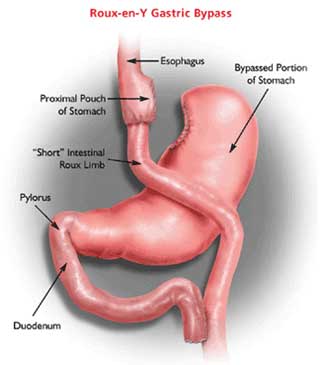
* Gastric bypass: The top portion of the stomach is cut and stapled to create a small pouch. The rest of the stomach and the first portion of the intestines are then re-routed. The patient can eat only small portions, and some of the food does not get absorbed. This is the most invasive of the bariatric surgeries.
* Sleeve gastrectomy: About 80 percent of the stomach is taken out, creating a small, banana-like sleeve. It allows patients to eat less and feel less hungry because the procedure removes some hormones that signal hunger. This is the newest of the bariatric surgeries.
Source: Dr. Jaime Ponce, medical director of the Gastric Band Institute
Labels: gastric bypass, gastric bypass research, gastric bypass risks, gastric bypass surgery education, weight loss