Stomaphyx: Gastric bypass pouch repair
Stomaphyx a novel approach to fixing a gastric bypass pouch that has stretched
San Antonio, TX
San Antonio, TX
Gastric Bypass Malpractice Attorney
Bariatric surgery has been a real boon for patients who need to lose massive amounts of weight. But sometimes, the small pouches created by gastric bypass procedures expand. Now, there’s a new procedure to help fix that problem.
Claudia Sisk, 51, of San Antonio lost more than 80 pounds after her original bypass surgery several years ago, but her pouch began to expand and she started regaining unwanted weight.
“Now I see myself eating a little more than usual so that’s why I went back and asked what else, was there a way they could tighten this pouch and make it smaller,” Sisk said.
“Previously, we would have to go in and operate and make incisions on the skin,” explained Dr. Mickey Seger, a bariatric surgeon. “It’s a very high risk operation. There’s over a 40% chance of having a problem or a complication with a re-do surgery like that.”
At Methodist Specialty and Transplant Hopsital, Sisk had a new procedure called Stompahyx. No cuts in the abdomen. The surgeon uses an endoscope to look down into the pouch, and a special tool to make it smaller.
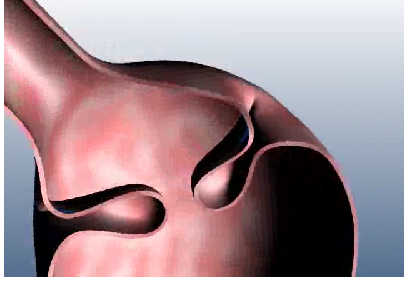
Here’s how it works. The instrument is guided into the stomach. A vacuum sucks a small piece of tissue into the tube, and then the device injects a fastener into place, creating a fold in the stomach. A series of folds literally closes down the pouch, making it harder for the patient to overeat.
“It’ll dramatically reduce the amount of food she can take before being full,” Seger said. “Whereas now she can eat pretty much a regular-sized meal, we’ll be able to get her satisfied with less than a cup.”
The procedure takes less than an hour. There are no cuts and no scars. Sisk is hopeful this novel approach will be the help she needs to achieve her goal.
“Hopefully, I’ll get under 200,” Sisk stated. “I want to be, you know, 180 to 200.”
There is no big recovery with this procedure. Patients are out of the hospital within 24 hours and back to work almost immediately. The idea is that they’ll start losing weight once again.
Labels: gastric bypass revision, StomaphyX