Cervical cancer vaccine: Older woman are not as likely to benefit from HPV vaccine
Older Women Are Not Likely to Benefit From Cervical Cancer Vaccine
New York, NY
New York, NY
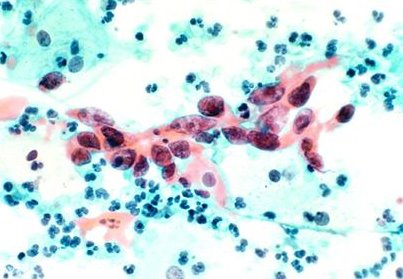
Women older than 40 are unlikely to get much benefit from the vaccine for the virus that causes cervical cancer, a new study reports.Cervical Cancer Misread Pap Test Malpractice Attorney
The vaccine for human papillomavirus, or HPV, is recommended for women up to age 26 and girls as young as 9. To determine whether older women might be protected as well, the new study looked at patterns of HPV infection as women age, said Dr. Ana Cecilia Rodríguez, the lead author of the new paper, published online Feb. 15 in The Journal of the National Cancer Institute. The study followed more than 9,000 Costa Rican women ages 19 to 97, screening them for carcinogenic HPV infections and precursors to cervical cancer. The rate of newly detected infections dropped with age — to 13.5 percent in women 42 and older, from 35 percent in women 18 to 25. In younger and older women alike, new infections generally cleared up without treatment, usually within two years.
Although cervical cancer is more common in older than in younger women, it develops decades after the initial infection with a carcinogenic virus, explained Dr. Rodríguez, of the Inciensa Foundation, a Costa Rican health and nutrition institute, whose work was supported by the National Institutes of Health in the United States.
“Because the HPV vaccine can only prevent infections, and these women are not getting that many new infections, the potential benefit of HPV vaccination among older women is very limited,” she said.
Labels: Cervical Cancer Research, HPV Vaccine